Clinical Knowledge Base
Insights on habit tracking as a clinical tool for engagement, retention, and compliance.
 Latest
Latest How to Stop Smoking Weed: A Realistic Guide
Quitting cannabis is harder than most people expect, not because it's physically brutal, but because it's quiet about it. Here's what actually helps.
Read article
Trump Signs Psychedelics Executive Order: What It Means for Harm Reduction, and Why Some Are Still Left Behind
Trump's April 2026 executive order on psilocybin, MDMA, ibogaine, and LSD marks a quiet turning point for harm reduction in the US. But not every substance, and not every user, made it into the frame. Here's what clinicians need to understand.
Read article
Measurement-Based Care for Addiction: What It Is, Why It Works, and How to Actually Use It
Clinicians who rely on memory and in-session self-report are flying blind between appointments. Here's what the evidence says about MBC in addiction treatment, and how to actually implement it.
Read article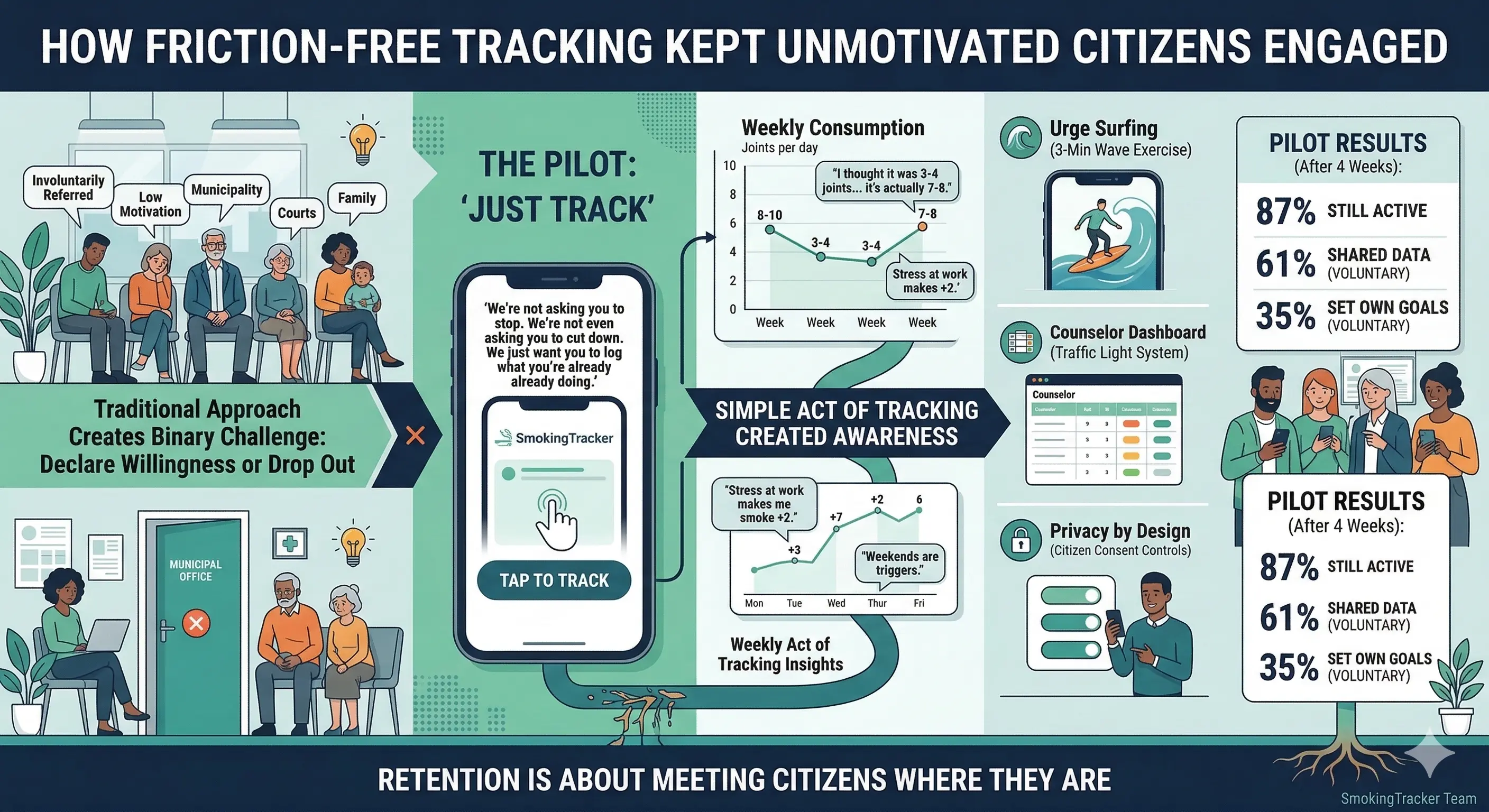
How Friction-Free Tracking Keeps Unmotivated Clients Engaged
Asking involuntary clients to 'just track' (without any pressure to change) is one of the most underused retention strategies in outpatient treatment. Here's why it works.

HIPAA, 42 CFR Part 2, and Client-Owned Addiction Data
Why giving clients full control over their substance use data isn't just legally required under HIPAA and Part 2, it's clinically superior.
Nicotine and Cannabis: When You're Treating Two Addictions at Once
When a client rolls cannabis with tobacco, you're not treating one addiction. You're treating two. Most treatment plans only address one of them.
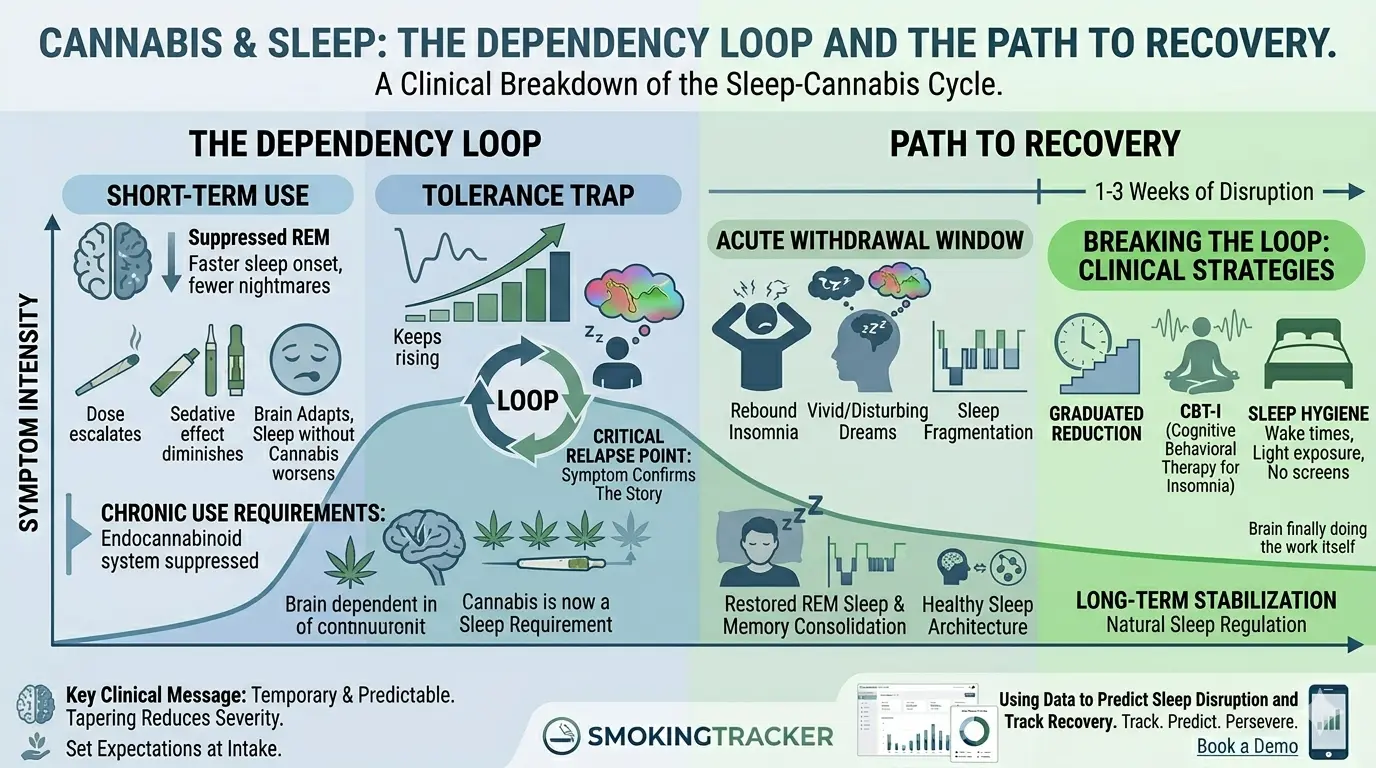
Cannabis and Sleep: Which Comes First?
Almost every cannabis client will tell you they need it to sleep. They're not wrong, and that's exactly the problem. A clinical breakdown of the sleep-cannabis dependency loop.
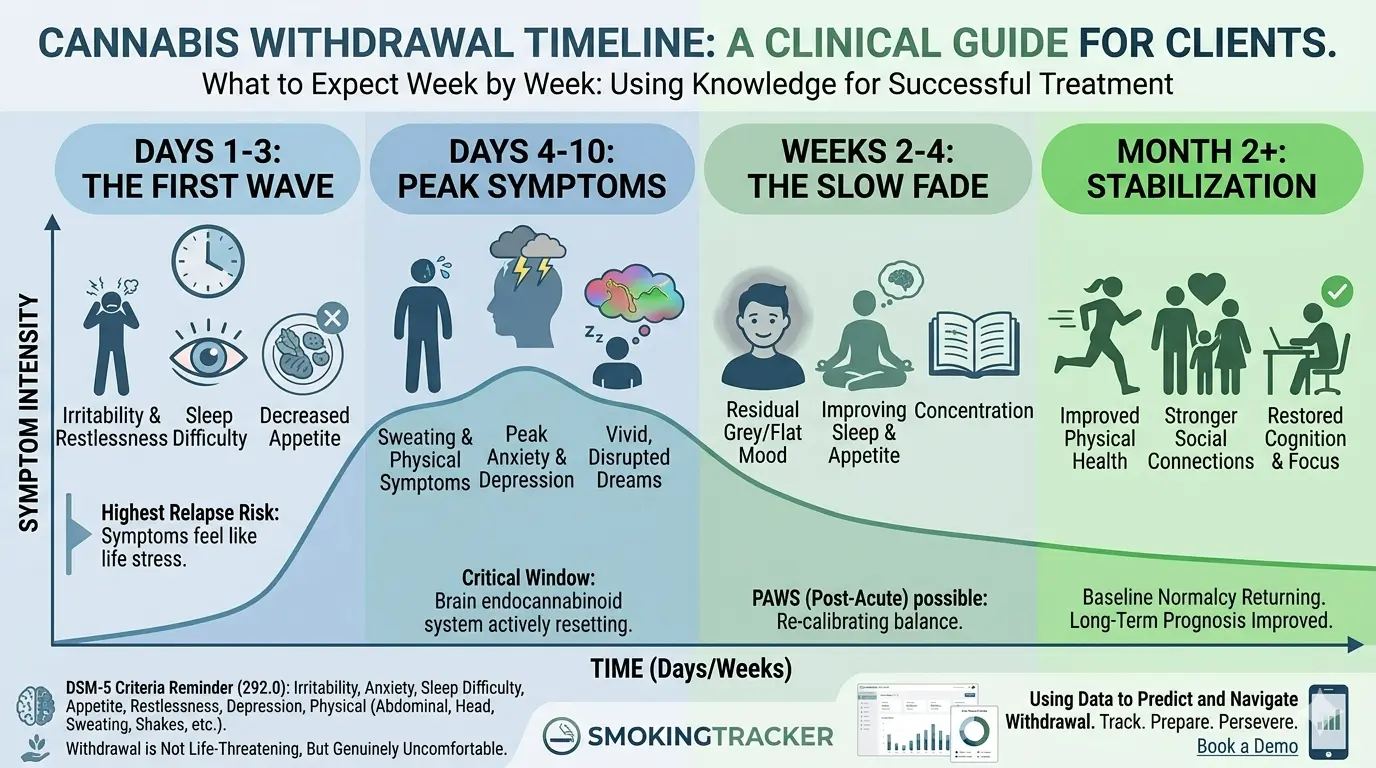
Cannabis Withdrawal Timeline: What to Tell Your Clients
Cannabis withdrawal is a recognized DSM-5 diagnosis with a predictable timeline. Here's what to expect week by week, and how to use that knowledge in treatment.
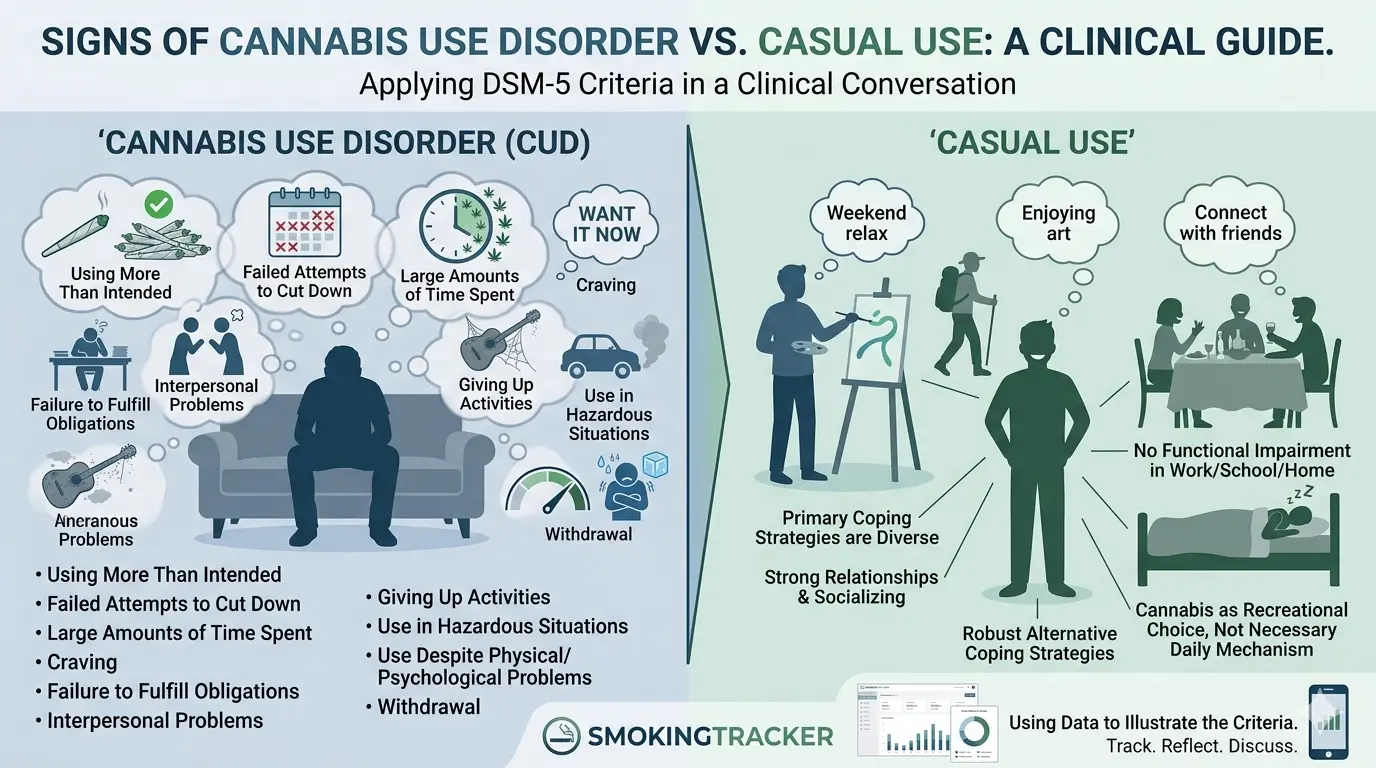
Signs of Cannabis Use Disorder vs. Casual Use: A Clinical Guide
Most clients will tell you they're casual users. The DSM-5 disagrees with at least some of them. Here's how to apply the criteria in a real clinical conversation.

Flower vs. Hash: What Counselors Should Know About Cannabis Forms
A deep dive into cannabis flower (bud), the difference between Indica and Sativa, and how different terpenes affect the client's experience.

Beyond THC: What Hash Color Tells You About a Client's High
Understand the connection between hash color, trichomes, and the chemical profile, and why dark hash often means a heavy, sedative experience for clients.