Cannabis Use Disorder (CUD) is a DSM-5 clinical diagnosis requiring at least 2 of 11 criteria within a 12-month period, including failed attempts to cut down, continued use despite problems, and withdrawal symptoms. An estimated 9% of people who try cannabis develop CUD, rising to 17% of those who start in adolescence (NIDA, 2020). As of 2022, approximately 4.3 million Americans met diagnostic criteria (SAMHSA NSDUH, 2022).
Most clients who end up in your office because of cannabis will tell you the same thing: they’re not addicted, they just like it. It’s not like alcohol. It’s not like meth. They can stop whenever they want, they just don’t want to right now.
That framing isn’t entirely dishonest. But it’s also not the full picture. Cannabis Use Disorder (CUD) is a recognized DSM-5 diagnosis, and the line between heavy casual use and a clinical disorder is more concrete than most clients (or some clinicians) realize.
The challenge isn’t the diagnostic criteria themselves. It’s applying them in a conversation where the client has already decided the answer is “no.”
The 11 DSM-5 Criteria, What They Actually Look Like
Despite its prevalence, CUD is significantly undertreated: only about 10% of people who meet the diagnostic criteria for CUD receive any form of treatment in a given year (SAMHSA NSDUH, 2022). This gap is partly explained by client denial, but also by the clinical challenge of applying criteria in a conversation where the client has already decided the answer is “no.”
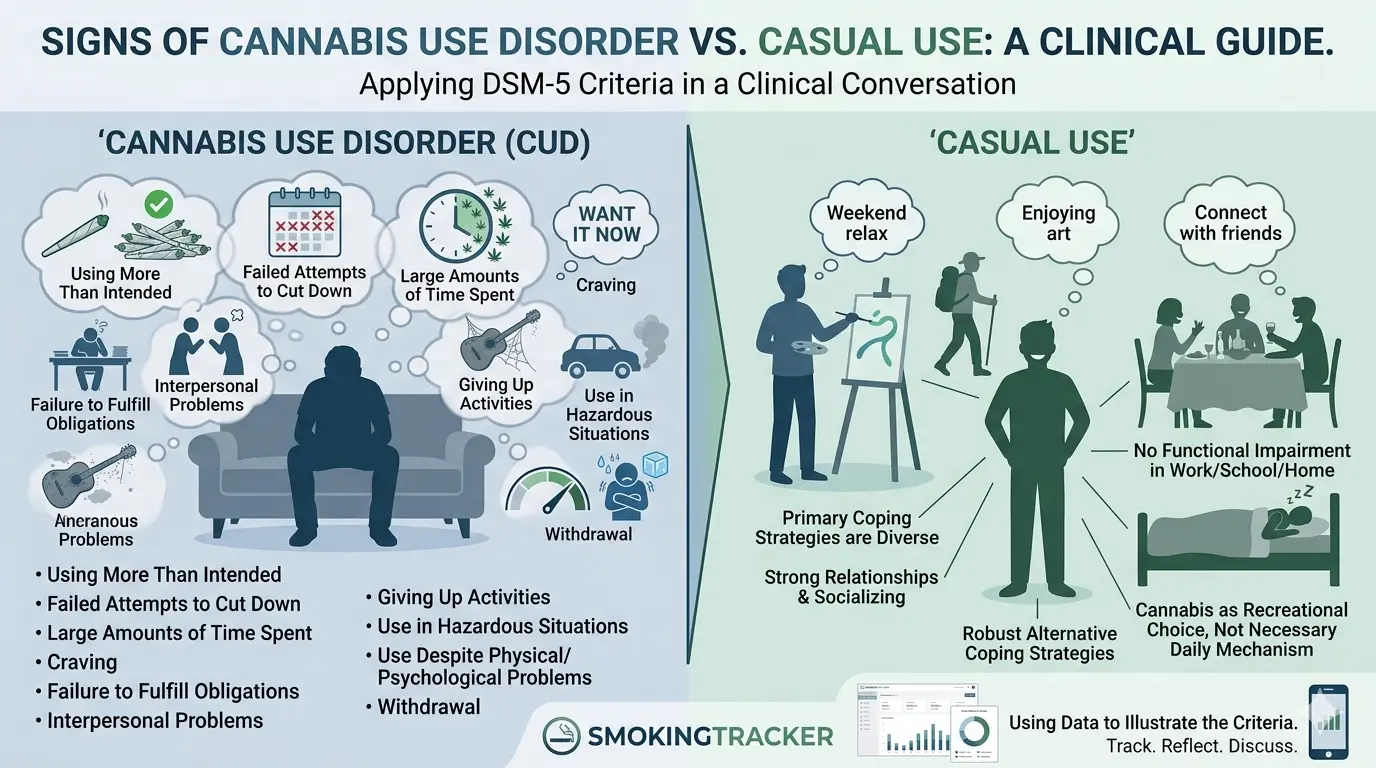
DSM-5 requires at least 2 of the following 11 criteria within a 12-month period to meet the threshold for Cannabis Use Disorder. Mild: 2–3 criteria. Moderate: 4–5. Severe: 6 or more.
1. Using more than intended. “I was just going to smoke one joint, but I ended up finishing the whole bag.” Clients often don’t recognize this as a criterion; they chalk it up to the quality of the product.
2. Persistent desire or failed attempts to cut down. “I’ve tried cutting back a bunch of times but it never sticks.” This is one of the most diagnostically significant criteria and also the one clients are most willing to acknowledge once you ask directly.
3. Large amounts of time spent obtaining, using, or recovering. This often presents as structuring the entire day around smoking: waking and baking, midday sessions, unwinding at night. The client may not see the time investment because it feels normal.
4. Craving. A strong desire or urge that is difficult to suppress. Clients may describe this as just “really wanting to smoke” rather than a craving, because craving is associated with harder drugs in their mental model.
5. Failure to fulfill major role obligations. Late to work, calling in sick, missing family commitments. Clients often minimize this: “I still get everything done, it just takes a little longer.”
6. Continued use despite social or interpersonal problems. Arguments with a partner about the habit. Tension with family. Withdrawing from friends who don’t smoke. The cannabis is causing friction, and they know it.
7. Giving up important activities. Hobbies, exercise, socializing sober. Often happens gradually and goes unnoticed until pointed out.
8. Use in physically hazardous situations. Driving high is the most common example. Many clients normalize this completely.
9. Use despite knowing it causes or worsens a physical or psychological problem. “I know it makes my anxiety worse but it also calms me down.” This ambivalence is clinically significant.
10. Tolerance. Needing significantly more to achieve the same effect. This criterion is often missed because it develops slowly over years and clients simply adjust without noticing.
11. Withdrawal. Recognized in DSM-5 since 2013. Irritability, anxiety, sleep disruption, decreased appetite within a week of stopping. Many clients have experienced this and attributed it to stress or “just being in a bad mood.”
The Casual Use Defense (and How to Respond to It)
When you raise the DSM criteria, you’ll encounter a predictable set of objections. The goal isn’t to win an argument, it’s to plant a seed of curiosity.
“I only smoke on weekends.” Frequency alone doesn’t determine disorder. A client who spends every Friday anticipating the weekend, modifies plans to ensure supply, and is irritable until they can smoke on Saturday afternoon may meet several criteria regardless of the day count.
“I can stop whenever I want.” The clinical response isn’t to challenge this, it’s to get curious: “That’s great. Have you tried recently?” If they have and found it harder than expected, that opens the door. If they haven’t tried in years, the confidence itself is worth exploring.
“It’s legal now.” Legal status is irrelevant to diagnostic criteria. Alcohol is legal. The question isn’t legality, it’s impact. Reframe toward function: “Legal or not, I’m interested in whether it’s working for you the way you want it to.”
Frequency vs. Function
The most useful clinical lens isn’t how much or how often, it’s what cannabis is doing for the client.
Is it the primary strategy for managing anxiety? The only way they can sleep? The thing they reach for immediately when anything stressful happens? That pattern of function (cannabis as a coping mechanism rather than a recreational choice) is where the disorder lives, regardless of frequency.
A client who smokes heavily every weekend but has strong alternative coping strategies, strong relationships, and no functional impairment is in a fundamentally different position than a client who smokes a smaller amount but has organized their entire emotional life around it.
The question to ask: “What would be different about your week if you couldn’t smoke?” The answer is almost always more revealing than any consumption log.
When Tolerance Hides the Severity
High-tolerance clients present a specific clinical challenge: they’ve adapted so thoroughly to their use level that they don’t experience it as excessive. They’re not lying when they say they feel fine; they’ve recalibrated their baseline.
The tell is often in the quantities. A client who has gone from a gram a week to an eighth a day over three years without noticing the escalation has profound tolerance, and almost certainly physical dependence, even if their daily functioning looks intact from the outside.
This is worth exploring directly: “When you first started, how much did it take to feel the effect? And how much does it take now?” The math of tolerance is often the first objective evidence that cuts through the “casual user” framing.
Frequently Asked Questions
What is Cannabis Use Disorder? Cannabis Use Disorder is a DSM-5 clinical diagnosis (code 304.30) characterized by a problematic pattern of cannabis use causing significant impairment or distress. It requires at least 2 of 11 criteria within 12 months, including tolerance, withdrawal, failed attempts to cut down, and continued use despite social or health problems.
How is Cannabis Use Disorder different from heavy cannabis use? The distinction is functional, not quantitative. Heavy use describes how much or how often someone uses cannabis. CUD describes what the use is doing to the person’s life: whether it’s impairing their relationships, obligations, or health, and whether they’ve lost control over the pattern. A person can use heavily without having CUD, and can have CUD with less frequent use.
How common is Cannabis Use Disorder? Approximately 9% of people who try cannabis develop CUD at some point. The rate is higher among daily users (estimated 25–50%) and among those who start in adolescence (up to 17%). In the US, about 4.3 million people met criteria for CUD in 2022, making it the most common illicit drug use disorder after alcohol.
Can you have Cannabis Use Disorder if cannabis is legal in your state? Yes. Legal status is clinically irrelevant to the diagnosis. Alcohol is legal and Alcohol Use Disorder is a recognized condition with the same DSM-5 framework. The criteria assess functional impairment and loss of control, not legality. Many clients use the legalization argument as part of the “casual user” defense; the clinical response is to redirect to function rather than engage the legal question.
What’s the first step in diagnosing CUD in a resistant client? The most productive approach is exploring the 11 DSM-5 criteria through open-ended questions rather than presenting the checklist directly. Asking “Have you ever tried to cut back and found it harder than you expected?” often opens more than any direct diagnostic framing. The goal in early sessions is to plant curiosity, not deliver a verdict. Once a client is open to the conversation about what comes next, Avenues Recovery’s overview of marijuana addiction treatment options is a useful patient-facing reference for talking through pathways.
This article was written by SmokingTracker, drawing on peer-reviewed research in cannabis use disorder treatment.
In SmokingTracker, clients log each session over time: frequency, quantity, time of day, and mood before and after. After a few weeks, the data often illustrates the DSM criteria more concretely than any clinical conversation can. When a client can see their own “failed attempts to cut down” in a chart, the diagnosis stops being something you’re imposing on them and starts being something they’re recognizing in themselves. Book a demo to see how tracking changes the diagnostic conversation.