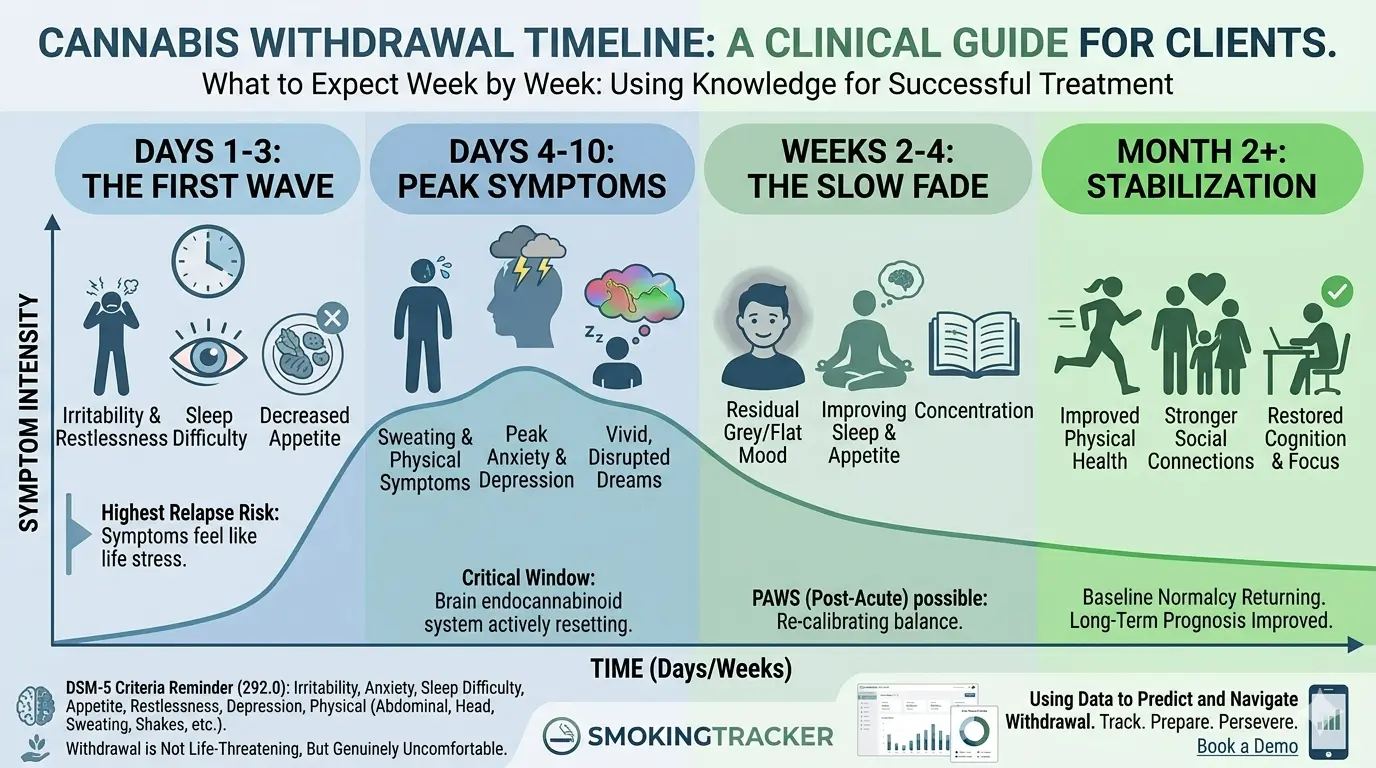
Cannabis Withdrawal Syndrome is a DSM-5 recognized condition (code 292.0) that occurs when a regular cannabis user stops or significantly reduces use. Symptoms (including irritability, anxiety, sleep disruption, and appetite loss) typically begin within 24–72 hours of last use, peak around days 4–10, and resolve over two to four weeks for most clients.
“I can quit whenever I want, weed isn’t addictive.”
Clinicians hear this constantly. And while the response used to be somewhat ambiguous, it no longer is. DSM-5 formally recognized Cannabis Withdrawal in 2013 (292.0), and the clinical picture is consistent enough that knowing the timeline gives you a real tool in treatment planning.
The goal isn’t to use withdrawal as a scare tactic. It’s to set accurate expectations so clients don’t interpret normal symptoms as proof that they need cannabis, which is the single most common driver of early relapse.
Is Cannabis Withdrawal Real? (The Short Answer: Yes)
Cannabis withdrawal is more prevalent than many clinicians expect. Research finds that approximately 47% of daily cannabis users report clinically significant withdrawal symptoms when they attempt abstinence (Budney et al., 2004, Drug and Alcohol Dependence). Among clients in treatment specifically for cannabis use disorder, the figure is higher, with sleep disruption reported in up to 76% of cases during the first week of abstinence (Haney, 2005, Psychopharmacology).
DSM-5 requires at least 3 of the following symptoms within one week of stopping or significantly reducing use: irritability or aggression, nervousness or anxiety, sleep difficulty, decreased appetite or weight loss, restlessness, depressed mood, and at least one physical symptom (abdominal pain, shakiness, sweating, fever, chills, or headache).
Notice what’s not on that list: seizures, hallucinations, or the kind of acute medical danger associated with alcohol or benzodiazepine withdrawal. Cannabis withdrawal is not life-threatening. But it is genuinely uncomfortable, and that discomfort is what sends clients back to using before they’ve given abstinence a real chance.
The other thing worth noting: many clients have already experienced withdrawal without recognizing it. The irritability after a few days without cannabis, the nights of poor sleep, the anxiety that spikes; they’ve filed these experiences under “just stress” or “bad week.” Naming it changes the clinical conversation.
Days 1–3: The First Wave
Withdrawal symptoms typically begin within 24–72 hours of the last use, and this opening window is the most dangerous in terms of relapse risk.
The dominant symptoms in days 1–3 are psychological: irritability, restlessness, and anxiety. Clients often describe a low-grade agitation they can’t pin to anything specific. Sleep becomes difficult, either taking longer to fall asleep or waking through the night. Appetite drops.
The clinical challenge here is attribution. Clients are more likely to interpret these symptoms as “life stress” or “why I need cannabis in the first place” rather than as withdrawal. This is where psychoeducation at intake pays off: “In the first few days, you’ll probably feel irritable and have trouble sleeping. That’s withdrawal, not evidence that you need it.”
Days 4–10: Peak Symptoms
If days 1–3 are the warning shot, days 4–10 are when withdrawal peaks for most clients.
Sleep disruption is at its worst. The brain, which has suppressed REM sleep under chronic cannabis use, rebounds sharply, producing vivid, often disturbing dreams that fragment sleep throughout the night. Clients who haven’t been warned about this are frequently blindsided by it and interpret the experience as a sleep disorder requiring cannabis to treat.
Mood instability is highest in this window. Some clients experience real depressive episodes; others experience a pronounced anhedonia, a flat, colorless quality to daily life that makes abstinence feel pointless. Physical symptoms (sweating, headaches, gastrointestinal discomfort) are most common in this period as well.
Clinically, this is the window that determines outcomes. Clients who make it to day 10–14 with support and accurate expectations have substantially better long-term prognosis than those who relapse in the acute phase. Every contact you have with a client in this window matters.
Weeks 2–4: The Slow Fade
For most clients, the acute symptoms begin resolving after the first week. Sleep improves, appetite returns, the sharpest edge comes off the mood disruption.
What can persist is subtler: a low-grade anxiety, difficulty concentrating, and a kind of emotional flatness that lingers for weeks. This is sometimes described as Post-Acute Withdrawal Syndrome (PAWS), though the evidence base for this as a distinct clinical entity in cannabis is still developing. What’s clinically consistent is that the brain’s endocannabinoid system takes time to recalibrate, and clients should be told to expect that “normal” doesn’t return overnight.
The risk in this phase is different from the acute phase. Clients aren’t fighting urgent discomfort; they’re fighting a grey, unmotivated baseline that makes the ease of resuming use look appealing by comparison. Boredom and anhedonia are the primary relapse triggers weeks 2–4, not acute craving.
What This Means for Treatment Planning
Set the timeline at intake, not after the fact. Clients who know what’s coming can contextualize their experience. Clients who are surprised by it interpret symptoms as evidence they need cannabis.
Sleep is a treatment variable, not a side issue. The disruption in weeks 1–2 is significant enough that sleep hygiene, CBT-I (Cognitive Behavioral Therapy for Insomnia), or melatonin support are worth addressing directly. Clients who don’t sleep don’t stay in treatment.
Increase contact in days 4–10. This is when clients are most likely to relapse and most likely to benefit from a check-in. A brief session or even a phone call during peak withdrawal has disproportionate impact on retention.
Normalize PAWS without catastrophizing it. “The first few weeks will be hard. Weeks 2–4 will be easier but still grey. By month 2, most people feel a lot better” is accurate, honest, and gives clients something to aim for. For clients who want a layperson-friendly read on what they’re going through, Avenues Recovery’s marijuana withdrawal explainer covers the same territory in non-clinical language.
Frequently Asked Questions
When does cannabis withdrawal start? Symptoms typically begin within 24–72 hours of the last use. The opening window (days 1–3) carries the highest relapse risk because clients misattribute the discomfort to stress rather than withdrawal. Setting expectations at intake is the most effective intervention for this phase.
How long does cannabis withdrawal last? For most clients, acute symptoms peak around days 4–10 and largely resolve by week 2–3. Subtler symptoms (low-grade anxiety, difficulty concentrating, emotional flatness) can persist for weeks as the endocannabinoid system recalibrates. Clients should be told to expect four to six weeks before feeling consistently normal.
What are the most common cannabis withdrawal symptoms? The DSM-5 criteria include irritability, anxiety, sleep difficulty, decreased appetite, restlessness, depressed mood, and at least one physical symptom (abdominal pain, shakiness, sweating, fever, or headache). Sleep disruption, particularly vivid dreams and fragmented sleep, is the symptom most likely to trigger relapse in the first two weeks.
Is cannabis withdrawal dangerous? Cannabis withdrawal is not medically dangerous. Unlike alcohol or benzodiazepine withdrawal, there is no risk of seizures or acute physiological crisis. It is, however, genuinely uncomfortable, and the discomfort is the primary driver of early relapse for most clients. Psychoeducation and clinical support during the acute phase meaningfully improve outcomes.
What is Post-Acute Withdrawal Syndrome (PAWS) in cannabis? PAWS refers to a prolonged phase of sub-acute symptoms (low motivation, difficulty with emotional regulation, and mild cognitive fog) that can persist weeks to months after the acute withdrawal resolves. The evidence base for cannabis PAWS as a distinct clinical entity is still developing, but the pattern of extended recovery is clinically consistent and worth naming to clients.
This article was written by SmokingTracker, drawing on peer-reviewed research in cannabis use disorder treatment.
In SmokingTracker, clients log session frequency alongside mood data throughout the reduction or cessation process. When a client is in the acute withdrawal window, the mood timeline in their data often shows the dip clearly, and the gradual improvement that follows gives clinicians a concrete way to show clients that the discomfort is temporary, not permanent. Book a demo to see how withdrawal tracking works in practice.