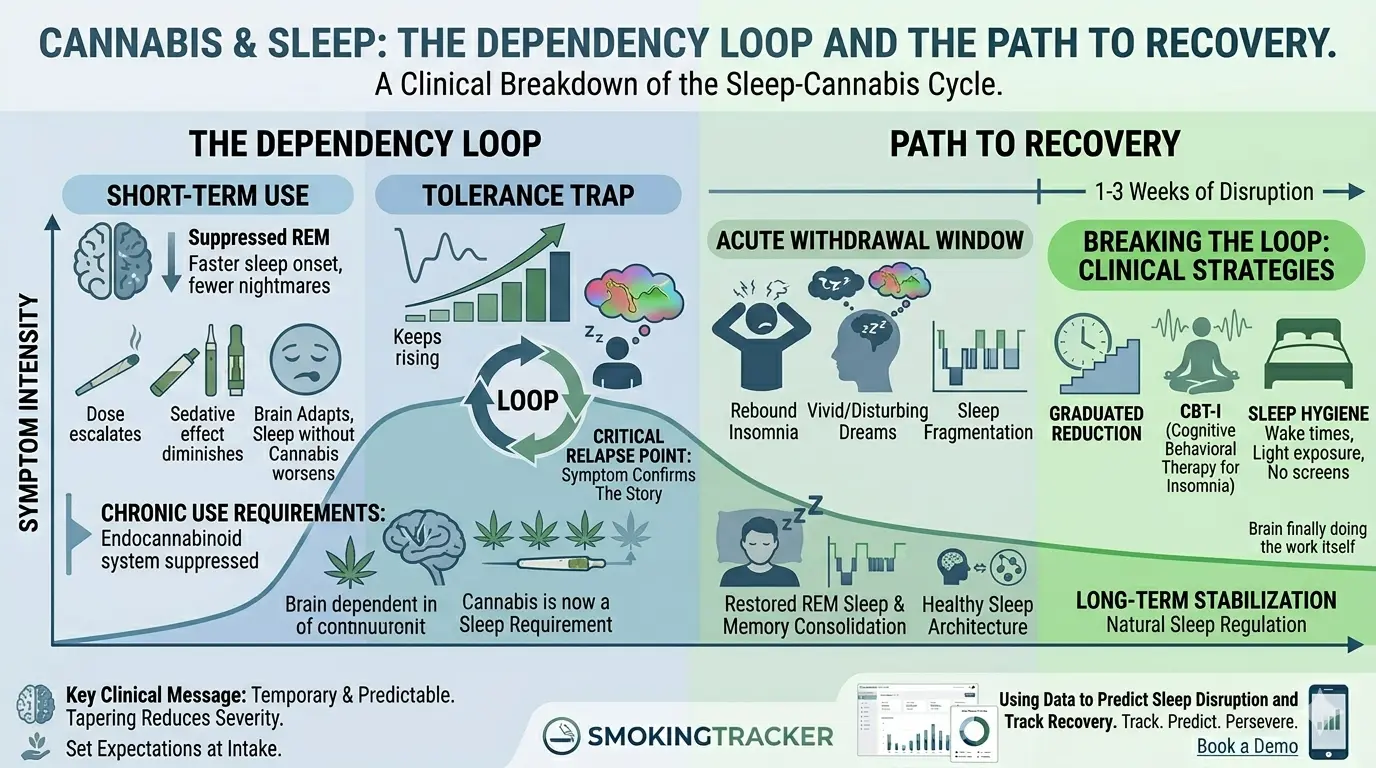
The cannabis-sleep dependency loop is a pattern in which short-term improvements in sleep onset become long-term dependence, as the brain suppresses its natural sleep regulation in response to chronic THC exposure. Research shows THC reduces sleep onset latency in the short term, but rebound insomnia during abstinence is reported in up to 70% of cannabis-dependent patients (Budney et al., 2011) and is the most commonly cited trigger for early relapse.
Almost every cannabis client will tell you they need it to sleep. They’re not wrong, and that’s exactly the problem.
Cannabis genuinely works as a short-term sleep aid. That’s not client rationalization; it’s pharmacology. The issue is what happens over months and years of use, and what happens when the client tries to stop. Understanding the sleep-cannabis loop is one of the most practically useful things a clinician can bring to a cannabis treatment case, because sleep disruption is the most commonly cited reason for relapse, and most clients have never had it explained to them.
Why Cannabis “Works” for Sleep
THC reduces sleep onset latency. Put plainly: it helps people fall asleep faster. A 2017 review in Current Psychiatry Reports (Babson, Sotile & Morabito) found meaningful reductions in time-to-sleep for short-term users, an effect that is real, consistent, and the primary reason clients develop confidence in cannabis as a sleep tool. For someone lying awake with an anxious or restless mind, that effect is real, immediate, and reinforcing.
THC also suppresses REM sleep, the stage associated with dreaming, emotional processing, and memory consolidation. For clients with trauma histories, this can feel like a clear benefit. Fewer nightmares, less emotional residue from sleep. For a client who has been woken by disturbing dreams for years, the appeal of a substance that reliably suppresses that experience is completely understandable.
The short-term efficacy is real, which makes the relationship feel self-evident to the client: cannabis helps me sleep, therefore I need cannabis to sleep. The therapeutic challenge is that this logical chain skips over everything that happens in between.
The Tolerance Trap
The same tolerance dynamics that apply to cannabis’s psychoactive effects apply to its sedative effects. Over time, the same dose that reliably induced sleep starts to feel insufficient. The client escalates: a bit more before bed, a higher-potency product, an additional session closer to lights out.
Meanwhile, something more meaningful is happening underneath. Chronic THC exposure suppresses the brain’s endocannabinoid system activity, including the systems involved in natural sleep regulation. The baseline (sleep without cannabis) gets progressively worse as the brain adapts to operating with external THC. What started as a sleep aid has become a sleep requirement.
This shift usually happens gradually enough that clients don’t notice it. They don’t think “I’ve become dependent on cannabis to sleep.” They think “I’ve always had trouble sleeping, and cannabis is what works for me.” Both things are partially true, which is what makes the conversation difficult.
Cannabis Withdrawal and Rebound Insomnia
When a client tries to stop or sharply reduce, the suppressed REM sleep rebounds. The brain, suddenly without the chemical suppression it has adapted to, overcorrects, producing intense, vivid, often disturbing dreams and fragmented sleep architecture for one to three weeks.
This rebound insomnia is probably the single most clinically significant factor in early cannabis relapse. The client isn’t being weak or unmotivated. They are unable to sleep normally, and they have an immediately available solution in the cabinet.
The clinical mistake is allowing this to happen without warning. A client who wakes up after two nights of disturbing dreams and total sleep fragmentation, with no context for why this is happening, will almost always conclude that their original belief was correct: they need cannabis to sleep. The symptom confirms the story.
A client who was told at intake (“When you stop, your sleep will get worse before it gets better. You’ll probably have vivid dreams and wake up more often for a week or two. That’s your brain readjusting, not proof that you need cannabis”) has a fighting chance of staying the course.
Breaking the Loop in Treatment
Graduated reduction often outperforms cold turkey for sleep-dependent clients. Abrupt cessation triggers the sharpest rebound. Tapering allows the endocannabinoid system to recalibrate more gradually, which reduces the severity of the sleep disruption window.
CBT-I (Cognitive Behavioral Therapy for Insomnia) should be a parallel intervention, not an afterthought. CBT-I has a stronger long-term evidence base for insomnia than any pharmacological intervention, including cannabis. The American Academy of Sleep Medicine designates CBT-I as the first-line treatment for chronic insomnia, with remission rates of 70–80% in clinical trials (Qaseem et al., 2016, Annals of Internal Medicine). Introducing it during treatment, even in a brief psychoeducational format, gives clients a legitimate alternative and builds the underlying sleep skills the cannabis has been substituting for.
Sleep hygiene is unsexy but it works. Consistent wake times, light exposure, temperature management, and stimulus control (not using the bed for anything other than sleep and sex) have meaningful impact. Clients often dismiss these as obvious or insufficient, but during the rebound period, they reduce the severity of the disruption.
Frame the disruption as temporary and predictable, not as a sleep disorder. The language matters: “Your sleep will be difficult for about two weeks. That’s the timeline. After that, most people sleep better than they have in years, because their brain is finally doing the work itself again.”
Frequently Asked Questions
Does cannabis actually help with sleep? Yes, in the short term. THC shortens sleep onset latency and suppresses REM sleep, which many clients find beneficial, especially those with trauma histories or anxiety. The problem is what happens over months of regular use: tolerance develops, the brain’s natural sleep regulation is suppressed, and sleep without cannabis becomes progressively worse.
Does cannabis affect REM sleep? Yes. THC suppresses REM sleep, the stage associated with dreaming, emotional processing, and memory consolidation. Short-term, this can feel like a benefit (fewer nightmares, less emotional residue). Long-term, REM suppression disrupts emotional regulation and memory. When use stops, the brain over-compensates with intense REM rebound, producing vivid dreams and fragmented sleep for one to three weeks.
What happens to sleep when you stop using cannabis? Rebound insomnia is the rule, not the exception, in the first two weeks of abstinence. The brain’s sleep systems have adapted to operating with external THC and need time to recalibrate. Sleep onset takes longer, dreams become vivid and often disturbing, and sleep quality is worse than before treatment began. This is temporary, but without warning, most clients interpret it as confirmation that they need cannabis.
How long does cannabis rebound insomnia last? For most clients, the most disruptive sleep disturbance resolves within one to three weeks of abstinence. Mild sleep difficulties (earlier wake times, occasional night waking) can persist for four to six weeks. Clients who receive psychoeducation at intake about the rebound timeline are much more likely to stay in treatment through this window.
Is CBT-I effective for cannabis-related insomnia? CBT-I is the evidence-based first-line treatment for chronic insomnia and is highly applicable to cannabis-related sleep problems. It addresses the behavioral and cognitive patterns that maintain insomnia independently of the original cause. For clients in cannabis treatment, introducing CBT-I principles (consistent wake times, stimulus control, cognitive restructuring) during the abstinence phase provides a real alternative to cannabis and builds lasting sleep skills.
This article was written by SmokingTracker, drawing on peer-reviewed research in cannabis use disorder treatment.
In SmokingTracker, clients log the timing of their sessions alongside mood data. Evening and late-night sessions become visible as a pattern over time, and that pattern often tells the clinical story more clearly than the client can. When a clinician can show a client “you smoked at 11pm every night for three weeks,” the conversation shifts from belief to evidence. Book a demo to see how session timing data changes the sleep conversation.